WITHOUT ORTHOTICS
OurHealthNetwork Articles
Custom-Made Dance Orthotics
During any repetitive weight-bearing activity, such as dancing, pressure is continuously applied to specific areas of the foot, rather than being equally distributed across the entire foot. All dance steps — whether you are ballroom dancing, swing or square dancing — cause tremendous forces to be applied to the balls of the feet, toes, arches, and ankles, and these structures are not constructed to bear these forces. Compounding these problems are inherent biomechanical abnormalities a dancer’s feet might have, such as pronation (a rolling out of the foot, so that you walk more on the inside border of the foot), supination (the opposite of pronation), a short leg, heel spurs, flat arches, very high arches, etc.
CUSTOM-MADE SPORTS ORTHOTICS
What are custom-made sports orthotics?
Custom-made sports orthotics are medical devices that allow the feet and ankles to function without pain, and to protect them from the repetitive stress of sports activities; or from just normal walking. They are designed and made from molds of your feet, constructed with comfortable "space age" materials, under the supervision of a Board Certified podiatrist who has 30 years of experience treating athletes.
|
|
WITH ORTHOTICS |
During midstance, the ankle and heel are misaligned, and your foot has no arch. |
At heel contact, orthoses limit the swing of your heel so your heel strikes the ground correctly. During midstance, your orthoses support your foot so it can regain its arch, allowing the ankle and heel to align. |
Drop Foot
- Description
-
Foot drop describes the inability to raise the front part of the foot due to weakness or paralysis of the muscles that lift the foot. As a result, individuals with foot drop scuff their toes along the ground or bend their knees to lift their foot higher than usual to avoid the scuffing, which causes what is called a “steppage” gait. Foot drop can be unilateral (affecting one foot) or bilateral (affecting both feet). Foot drop is a symptom of an underlying problem and is either temporary or permanent, depending on the cause. Causes include: neurodegenerative disorders of the brain that cause muscular problems, such as multiple sclerosis, stroke, and cerebral palsy; motor neuron disorders such as polio, some forms of spinal muscular atrophy and amyotrophic lateral sclerosis (commonly known as Lou Gehrig’s disease); injury to the nerve roots, such as in spinal stenosis; peripheral nerve disorders such as Charcot-Marie-Tooth disease or acquired peripheral neuropathy; local compression or damage to the peroneal nerve as it passes across the fibular bone below the knee; and muscle disorders, such as muscular dystrophy or myositis.
Diabetes
- Description
-
Diabetes is a disease that affects every part of the body, even when the diabetes is under control. Diabetics, because of the nature of their disease, have fewer defenses against everyday wear and tear, especially where the feet are concerned. Increased blood sugar affects the feet in the following ways:
The sugar affects the nerves of the feet, causing peripheral neuropathy. Peripheral neuropathy is a disease which can produce anything from strange feelings in the feet (burning, tingling, numbness, etc.), to a complete loss of feeling in the feet. The lack of proper feeling makes the diabetic more likely to injure their feet without knowing it. This makes the diabetic more susceptible to infections; fractures which are not felt, and do not heal properly; and severe bone and joint disease which changes the contour of the foot. See Charcot Foot for more information.
Sugar also affects the smaller blood vessels in the feet causing peripheral vascular disease (P.V.D.). P.V.D. decreases the amount of blood, nutrients, and oxygen that are brought to the skin, fat, muscles, joints, and bones of the feet. This causes: tissues to be absorbed, an inability to properly heal everything from small cuts to broken bones, and just plain fatigue and weakness of the feet.
Absorption of the natural protective fatty pad on the bottom of the feet. This is due to P.V.D. and/or the natural aging process. When the fat pad becomes thinned or completely absorbed, it cannot protect the skin properly from normal bone pressure. This puts tremendous stress on the skin which underlies these bones, and can cause inflammation, calluses, and eventually skin ulcers which may become infected. These problems may become worse without the diabetic knowing it, if peripheral neuropathy is present.
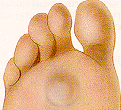
Calluses
The formation of calluses is caused by an accumulation of dead skin cells that harden and thicken over an area of the foot. This callus formation is the body’s defense mechanism to protect the foot against excessive pressure and friction. Calluses are normally found on the ball-of-the-foot, the heel, and/or the inside of the big toe. |
|
Bunions
What are bunions?
|
The common bunion is a localized area of enlargement of the inner portion of the joint at the base of the big toe. The enlargement actually represents additional bone formation, often in combination with a misalignment of the big toe. The misalignment causes the big toe to move outward (medically termed hallux valgus deformity). The normal position of the big toe (straight forward) becomes outward directed toward the smaller toes. The enlarged joint at the base of the big toe (the first metatarsophalangeal joint, or MTP joint) can become inflamed with redness, tenderness, and pain. A small fluid-filled sac (bursa) adjacent to the joint can also become inflamed (bursitis), leading to additional swelling, redness, and pain. A less common bunion is located at the joint at the base of the smallest (fifth) toe. This bunion is sometimes referred to as a tailor’s bunion. |

Arch Pain
The arch functions as a shock absorber for our entire body. Each time we step down, we place up to 5 times our body weight on the foot, depending on whether we are walking, running, or jumping. If there were no shock absorber in the foot, the force of each step would fracture or dislocate the bones of the foot, leg, and lower back. When pain occurs in the arch, it is telling us it is “sick” and cannot function properly. If left untreated, it can cause constant pain throughout the entire foot, and eventually the knee, hip, and lower back.
Achilles Tendonitis
DESCRIPTION & CAUSES
Achilles Tendonitis is an inflammation of the Achilles Tendon. This tendon attaches the muscles in the calf of the leg to the back of our heels. The Achilles Tendon is a long and thick tendon, which moves our foot down, so that the toes point to the ground (plantar flexion). This tendon can become inflamed due to the following causes:
Over utilizing it, such as too much running, especially up or down hill.
Trauma, such as a kick to the tendon.
Shoe or boot pressure, especially at its attachment to the heel, or just above it.
There are over 250,000 injuries to the Achilles Tendon annually. In fact, more Than 10% of all running injuries are to the Achilles tendon.
Tendonitis may be classified as either acute or chronic
Acute Achilles Tendonitis comes on quickly, usually after a specific activity or event. It is characterized by an overstretching or tearing of some of the small fibers of the tendon, and causes pain or tenderness when walking or running. It can occur at the insertion (near the attachment to the heel bone, or further up the leg, about 4 or 5 inches above the heel. Acute tendonitis can also follow a specific injury, such as a kick to the tendon while playing soccer.
Chronic Achilles Tendonitis develops gradually over time. Many times, you can feel an obvious thickening of the tendon that may be tender when squeezed, due to long standing scarring of the tendon. Pain is also present when walking or during other forms of activity, and feels better at rest.